
Class II Restorations complete procedure solution


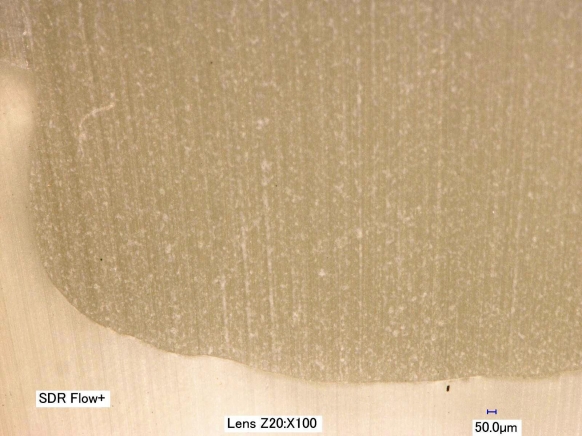
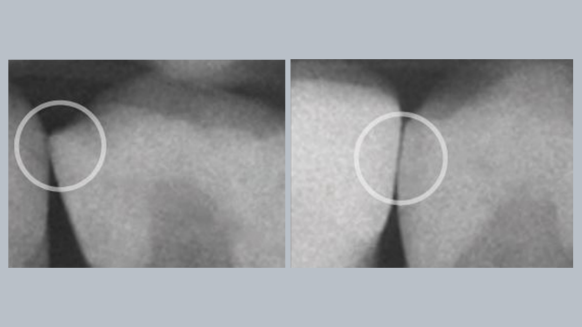
Uncertain of gap formation?
2 out of 3 dentists indicate cavity adaptation is the most important attribute for a successful restoration.2
You'll love SDR flow+ Bulk Fill Flowable!
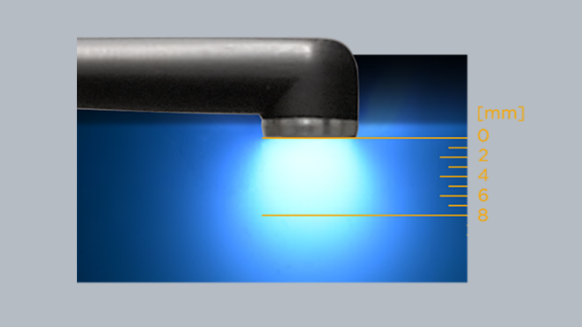
SDR flow+ material is a one-of-a-kind breakthrough in dentistry—a bulk fill flowable that combines exclusive self-leveling properties and category-best shrinkage stress—which allows for placement up to 4 mm with excellent cavity adaptation, enabling the placement of gap-free restorations.

The Dentsply Sirona Class II Approach has been the foundation of my posterior composite armamentarium and teaching protocols for more than 15 years. Using this system simplifies the protocol and enables the clinician to produce efficient and consistent successful outcomes without the stresses of complications and failures."
Navigating key challenges of Class II Restorations
It may be difficult to achieve your goals due to challenges associated with Class II restorations. Predictably and efficiently manage Class ll restorations to keep patients happy and your practice profitable. Learn more!





You want to know more about the Dentsply Sirona Class II Solution?
Submit your contact details and we will get in touch with you.
- DentalTown. Restorative dentistry monthly poll: What is the most challenging part of a Class II Restoration? 2012. For more information, contact Consumables-Data-Requests@dentsplysirona.com
- Key Group International Survey, 2019. For more information, contact Consumables-Data-Requests@dentsplysirona.com
- Dentsply Sirona Restorative, GNY 2016 Attendee Survey. For more information, contact Consumables-Data-Requests@dentsplysirona.com
- Internal data on file. For more information, contact Consumables-Data-Requests@dentsplysirona.com
- Usman AB, Ahmed A, Qasim J. Frequency of postoperative sensitivity in posterior class I composite restorations. Pakistan Oral Dent J. 2014;34(3):532-535. / Berkowitz GS, Horowitz AJ, Curro FA, et al. Postoperative hypersensitivity in class I resin-based composite restorations in general practice: interim results. Compend Contin Educ Dent. 2009;30(6):356-363. / Haller, Die postoperative Hypersensibilität, zm 99, Nr. 6a, 13.03.2009 S. 44-51./ Briso ALF, Mestrener SR, Delício G, et al. Clinical assessment of postoperative sensitivity in posterior composite restorations. Oper Dent. 2007;32(5):421-426. doi:10.2341/06-141
- BlueLight Analytics. Irradiance value comparison among commercially available curing lights. 2012. Unpublished commissioned study, data on file. For more information, contact Consumables-Data-Requests @dentsplysirona.com
- Internal data on file. For more information, contact Consumables-Data-Requests @dentsplysirona.com
- Perdigão J, Geraldeli S, Hodges JS. Total-etch versus self-etch adhesive: effect on postoperative sensitivity. JADA. 2003;134(12):1621-1629.
- Jackson RD. Placing posterior composites: increasing efficiency. Dent Today. 2011;30(4):126,128,130-131.
- Kuper NK, Opdam NJ, Ruben JL, et al. Gap size and wall lesion development next to composite. J Dent Res. 2014;93:108S-113S.
- Schneider LFJ, Cavalcante LM, Silikas N. Shrinkage stresses generated during resin-composite applications: a review. J Dent Biomech. 2010;131630. doi:10.4061/2010/131630
- Key Group International Survey, 2019, n=300. For more information, contact Consumables-Data-Requests@dentsplysirona.com
- Gilbert GH, Litaker MS, Pihlstrom DJ, Amundson CW, Gordan VV. DPBRN Collaborative Group. Rubber dam use during routine operative dentistry procedures: findings from the Dental PBRN. Oper Dent. 2010;35(5):491-499. doi:10.2341/09-287C
- DentalTown. Restorative Dentistry. Monthly poll: what is the most challenging part of a Class II restoration? 2012
- Rosenburg JM. Making contact: a method for restoring adjacent posterior direct resin. Dent Today. 2013;32(3):92,94-95
- Key Group International Survey, 2019, n=300. For more information, contact Consumables-Data-Requests@dentsplysirona.com.
- Jackson RD. Placing posterior composites: increasing efficiency. Dent Today. 2011;30(4):126,128,130-131.
- Kuper NK, Opdam NJ, Ruben JL, et al. Gap size and wall lesion development next to composite. J Dent Res. 2014;93:108S-113S. doi:10.1177/0022034514534262
- Data on file. Dentsply Sirona Restorative. GNY 2016 Attendee Survey. For more information, contact Consumables-Data-Requests@dentsplysirona.com
- Clinicians Report March 2021.
- Paul S, Peter A, Hämmerle CHF. Visual and spectrophotometric shade analysis of human teeth. J Dent Res. 2002;81(8):578-582.
- BlueLight Analytics. Irradiance value comparison among commercially available curing lights. 2012.
- Boksman L, Santos GC. Principles of light curing. Inside Dentistry. 2012;8(3). https://www.aegisdentalnetwork.com/id/2012/03/principles-of-light-curing