
Give us a call or provide your contact details below, and a Dentsply Sirona representative will be in touch soon.

Clinical Cases
Clinicians far and wide, throughout Australia and New Zealand kindly share relevant, interesting and sometimes challenging patient presentations, along with their selection of materials and methods to optimise their patients' outcomes.
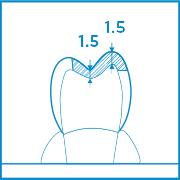
Indirect "Single Visit" CEREC Tessera Onlays
It is quite common to observe cracks and fractures associated with amalgam restorations, particularly as they increase in size as they are ‘unbonded’ restorations. Many of these teeth are structurally compromised and an adhesive, biomimetic approach is the ideal method of restoring these teeth. As a part of a more comprehensive treatment plan, this quadrant was planned to have two indirect ceramic onlays. The first and second molars were restored in a single visit using CEREC Tessera, an advanced lithium disilicate.
Dr Yo-Han Choi, Sydney, Australia
Conserving tooth structure through appropriate file selection
The patient presented with asymptomatic apical periodontitis on tooth 34. From the pre-op radiograph, tooth 34 was noted with two visible roots. However, a CBCT scan confirmed a three rooted premolar, and the canals divided into three at the mid root. A careful file selection is critical for this delicate tooth.
Dr Jack Lin, Endodontist, Sydney, NSW Australia
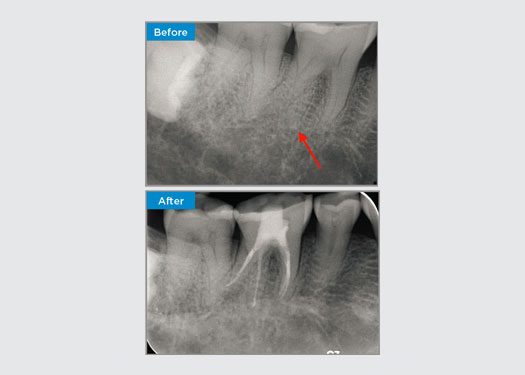
Irreversible Pulpitis on Tooth 46
In this situation, tooth/root structure preservation is essential to reduce the risk of ledging, transportation, zipping, perforation, and root fracture. Case selection, diagnosis, and pre-treatment planning are important. Endodontic file selection with flexibility, efficiency, and respect of natural root anatomy is critical.
The patient was presented with irreversible pulpitis on tooth 46. From the pre-op radiograph, tooth 46 is presented with an additional distal root (Radix Entromolaris tooth morphology). A CBCT scan has confirmed the presence of DL root with severe root curvature. A careful file selection is critical for this delicate DB root.
Dr Jack Lin, Endodontist, Sydney, NSW Australia

Root Canal Therapy on Tooth 16
A 35 year old female patient presented after referral from a Specialist Periodontist. During the initial endodontic assessment the patient mentioned crown lengthening had been performed, prior to placement of the crown on tooth 16, two years earlier. Two months prior to the patient presenting, she had noted swelling of the palatal gingiva. The patient’s general dental practitioner had discovered a 7mm periodontal pocket adjacent the palatal sinus tract associated with tooth 16. The patient was referrred to a Specialist Periodontist. The Specialist Periodontist diagnosed a primary endodontic - secondary periodontal lesion. The patient had satisfactory oral hygiene and was a regular dental attender. Tooth 16 was tender to percussion. It was noted that the crown margins were satisfactory and the periodontal pockets around tooth 16 were less than 2mm deep on the buccal aspect, however on the palatal surface, adjacent the sinus tract there was a 6.5mm isolated periodontal pocket. Thermal testing of tooth 16 revealed a negative response. Tooth 16 had risk factors for apical periodontitis such as: a negative response to thermal testing, tenderness to percussion, a history of a deep restoration following crown lengthening surgery and radiographically identifiable periapical disease. Tooth 16 did not have a history of pain on biting or chewing, which may indicate a crack communicating with the pulp and/or periodontal tissues. The patient had no risk factors for periodontal disease and there was no abnormally deep pocketing present around any other teeth.
Dr Omar Ikram, Endodontist, Crows Nest, NSW Australia

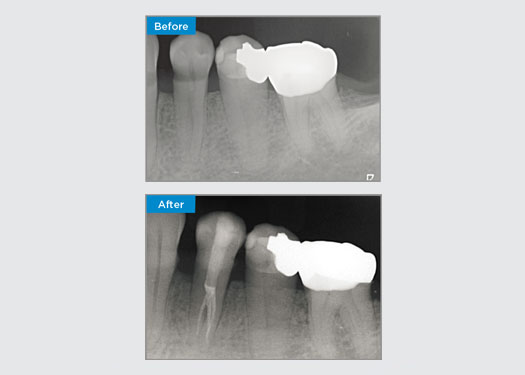
Indirect “Single Visit” Onlay
This patient presented with a broken restoration on tooth 46 distal-occlusal aspect. The tooth’s existing restoration extended very deep and close to the pulpal chamber. Given the large size of the restoration, it was highly likely that if we simply replaced the restoration with another direct restoration, the result would be the same, with the restoration breaking under the occlusal loads the tooth and restoration are subjected to. So an indirect option was recommended for the tooth. As the mesial third of the tooth was largely unaffected with substantial sound tooth structure remaining, we could preserve it and be minimally invasive by restoring the tooth with an indirect restoration using the CEREC system
Dr Sahil Soni, Queensland, Australia

Immediate Implant Placement and Immediate Definitive Restoration of a Maxillary Central Incisor
When considering the replacement of a maxillary central incisor with an implant-borne fixed dental prosthesis, case selection, planning and the meticulous application of treatment methods are the keys to success. Immediate implant placement and immediate restoration may minimise tissue loss and result in a highly aesthetic outcome. Implant placement with a fully-guided approach can improve the accuracy of placement, and the placement of the final abutment or restoration at the time of implant placement can promote tissue stability.
Dr Alan Yap, Prosthodontist, Sydney, Australia

Indirect “Single Visit” Onlay
Often patients are unaware of the cracks or cavities in their teeth. It is only when a tooth hurts, or breaks do most patients realise the need to get their teeth checked. Often, we can pre-empt things like teeth cracking, based on the presence of existing cracks, heavy occlusion or history of previous tooth loss due to a crack. In this case, the patient had an asymptomatic cracked upper premolar tooth which was picked up during a routine dental check up. The patient was shown the photograph of the tooth and made aware of the situation, with a recommendation to having the tooth restored. However, the patient declined any treatment as he was not experiencing any symptoms from the tooth. 6 months later, the tooth cracked and now the patient could not put off treatment any further. The tooth was restored using CEREC with a ceramic-resin hybrid crown/onlay in one visit.
Dr Sahil Soni, Queensland, Australia
At Dentsply Sirona, every day, we empower dental professionals all over the world to provide millions of patients with better dental care and make people smile. Our Clinical Case Spotlight is about sharing these smiles, that clinicians in Australia and New Zealand have created, with the greater dental community.
If you have a case that you would like to share, please email anz-communications@dentsplysirona.com
