Contents:
- Introduction
- The Role of Polymerisation Shrinkage and Shrinkage Stress in composite materials
- Addressing the Challenges of Composite Placement
- Introducing SDR® Bulk Fill Flowable Composite
- In vitro Studies on Polymerisation Shrinkage and Marginal Adaptation of SDR® Bulk Fill Flowable Composite
- Clinical Study Results
- Conclusion
SDR Bulk Fill Flowable Composite: The game changer for posterior composite restorations
Introduction:
The Rise of Composite Resin and Environmental Concerns about Amalgam
Over the past 40 years, composite resin has outpaced amalgam in dentistry extensively due to the demand for more aesthetic restorations worldwide. Additionally, environmental effects of dental amalgam resulted in either a decline or a ban in many countries and dental amalgam may eventually phase out in response to the Minamata convention.1
Composite Resin Failure and Risk of Secondary Caries
The problem with composite resins is that according to a recent systematic review, they have approximately double the failure rate of amalgam restorations.2 Restoration fracture does not seem to be greater with composite resin restorations, but the risk of developing secondary caries is significantly higher. The major questions when evaluating the aetiologies of failure are why there are more failures with composite than amalgam and what are the reasons for greater recurrent caries.
Addressing the Challenges with Composite Resin
Dental manufacturers have made developments in alternative materials, the composites resins, to address these questions with improvements in filler composition, photo-initiators, and mechanical properties to improve wear and durability.3,4
What are the Challenges:
The Role of Polymerisation Shrinkage and Shrinkage Stress
The process of photo-polymerisation results in the resin monomers connecting to make larger molecules called polymers which also join together forming a continuous network. However, the composite shrinks rapidly via this free radical process resulting in volumetric shrinkage in the range of 2-6% depending on the type of composite used. When the composite is placed in a deep preparation after adhesive placement and is photo-polymerised, it has a limited ability to relax and flow, creating stress within the material as well as the tooth-restoration interface that may result in debonding when the shrinkage stress is greater than the bond strength of the adhesive. Additionally, these stresses may continue and damage the restoration-adhesive interface during masticatory function.5 The net result is a plethora of clinical complications including cuspal deflection, enamel cracking and larger marginal gap formation leading to greater bacterial colonisation, secondary or recurrent caries, post operative sensitivity, pulpal inflammation and expedited failure.6 The common hypothesis for many years was that as photo-polymerisation was occurring, the composite was shrinking towards the light. However, additional studies over the years postulated the direction was the result of boundary conditions or the ratio of bonded to unbonded cavity walls (C-factor) and less affected by the relation toward the light.5,7,8
Addressing the Challenges:
Different Approaches to Composite Placement and Light Curing Protocols
Based on the complexities with polymerisation shrinkage, different approaches to composite placement have been proposed to reduce composite resin failure. Different light curing protocols such as soft-start, ramp cure and pulse delay have limited clinical evidence to suggest improved outcomes over the conventional light curing devices.5
The first-generation flowable composites were touted to suggest their low viscosity would create better adaptation to the dentine and help reduce effects of shrinkage based on their low modulus of elasticity. However, their elevated volumetric shrinkage from a low filler content and weak mechanical properties resulted in unfavorable clinical results compared to existing alternatives.9 Several incremental placement protocols were presented to reduce the C-factor by minimising the amount of composite in contact within the cavity walls and potentially allowing for more flow of the composite.
However, depending on the protocol used, incremental filling may not reduce polymerisation stress to the tooth.10 Another disadvantage of multiple increments of 4 or more, is the increased time to do the procedure. If not using a rubber dam, the error potential increases making the procedure more technique sensitive, less efficient and less proficient.
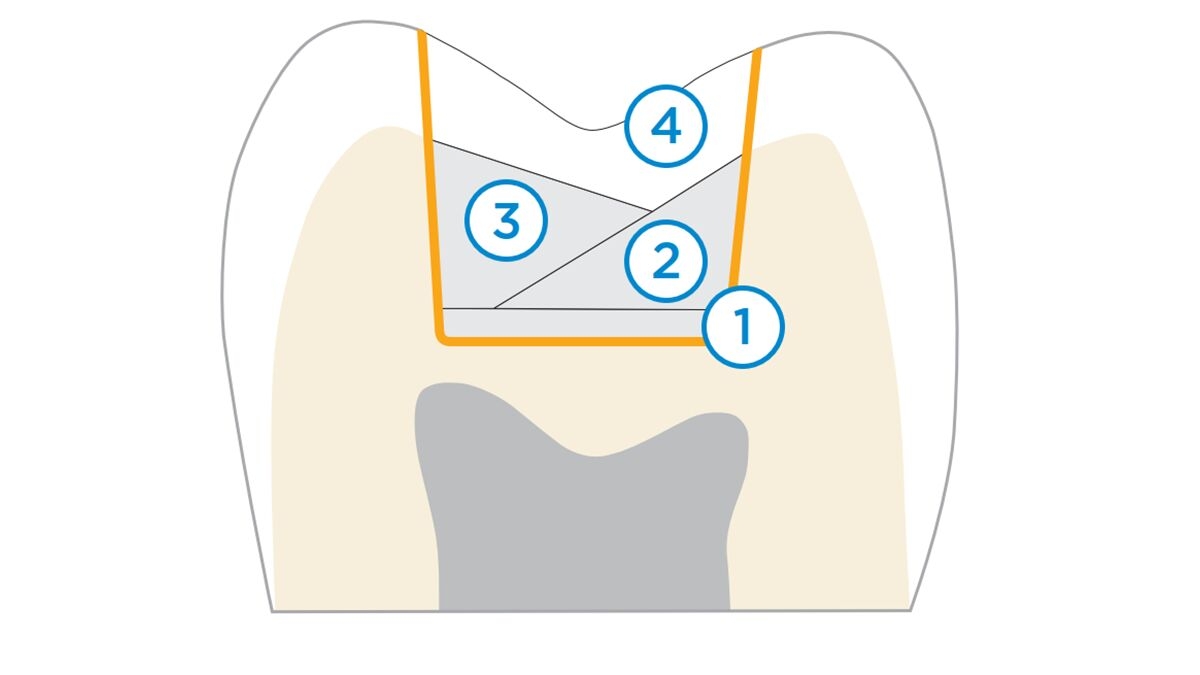
Illustration of a conventional layering approach for posterior composite restorations, consisting of an initial layer of flowable composite as liner (1), two triangular shaped layers of universal composite that aim at maximising the amount of unbonded composite surface to reduce shrinkage stress build-up (2+3) and a final occlusal capping (4).
Advances of Composites: Introducing Bulk-Fill materials
To answer this procedural risk, bulk-fill composite materials were introduced by dental manufacturers, starting in the late 1990’s (e.g. Surefil® Composite by Dentsply Sirona), to expedite the extended procedure times of incremental filling techniques and curing by modifying translucencies and photo-initiators, providing an enhanced depth of cure and thus allowing the placement of larger increments.
To manage shrinkage and stress build-up, those bulk-fill materials featured a high filler content, thereby minimising volumetric shrinkage, and consequently require the dental practitioner to pack the material into the cavity to create the required adaptation. More recent materials of this category of packable/sculptable bulk fill composites were stated to be able to be used in up to 5mm increments with lower polymerisation shrinkage stress due to decreased filler amount or increased filler size and incorporation of stress modifiers.11,12
Since 2009 however, bulk-fill composites have been subdivided into two groups based on viscosity. In addition to the high viscosity or packable/sculptable bulk-fills, low viscosity or flowable bulk-fills emerged as a new material category, with lower filler contents and weaker mechanical properties. Those materials are generally used as dentine replacements only requiring a 2mm enamel capping layer of traditional composite.12
The polymerisation shrinkage and polymerisation shrinkage stresses of both types of bulk-fill composites have been analysed and compared in several studies. 11,13,14,15,16,17,18,19,20,21,22,23
What was concluded and stood out prominently from all the studies referenced was that one flowable bulk-fill chemistry had the lowest polymerisation shrinkage stress - SDR® Bulk Fill Flowable Composite.
Introducing SDR® Bulk Fill Flowable:
Features and Handling Characteristics
SDR® Bulk Fill Flowable Composite is a one-component, fluoride-containing, visible light cured, radiopaque composite. SDR® Bulk Fill Flowable Composite has handling characteristics typical of a flowable composite, however, it can be placed in 4mm increments with minimal polymerisation stress. SDR® Bulk Fill Flowable Composite has a self-leveling feature that allows intimate adaptation to the prepared cavity walls.
When used as a base/liner material in Class I and II restorations, it is designed to be overlayed with a methacrylate-based universal/posterior composite for replacing missing occlusal/facial enamel. It is also suitable as a stand-alone restorative material in conservative Class I, Class III and V restorations without a separate capping being applied on top. To ensure aesthetic appearance in Class III and V restorations, the shade range has been expanded to A1, A2 and A3 shades in addition to the universal shade.
Lower Polymerisation Shrinkage Stress due to Unique UDMA Structure
The SDR® Bulk Fill Flowable Technology exhibits a patented urethane dimethacrylate structure (UDMA) that allows for a volumetric shrinkage of only 3.5%, which puts it on the low end in overall shrinkage compared to other flowable composites. Though lower volumetric shrinkage can contribute to overall lower polymerisation stress reduction, it is the polymerisation pattern and the patented and therefore unique UDMA structure that is key to stress reduction.
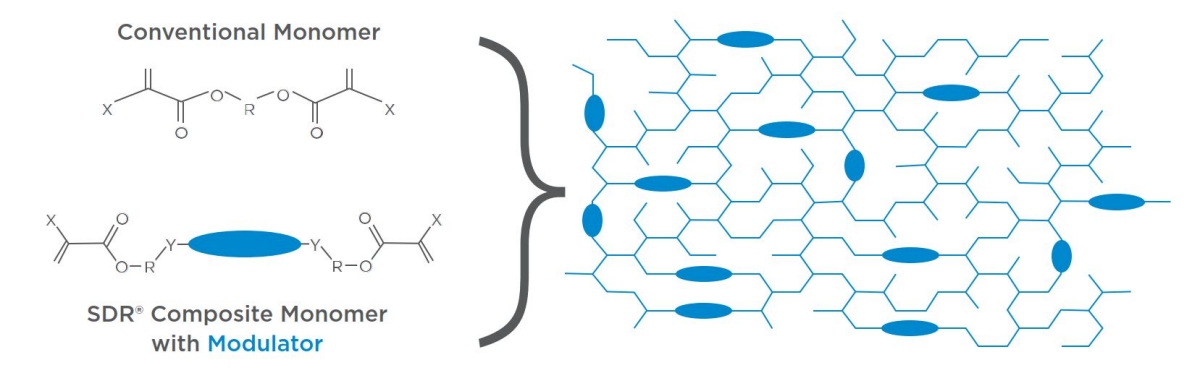
Compared to conventional resin systems, the SDR® Bulk Fill Flowable Composite forms large molecular structures upon polymerisation that, according to the manufacturer, include a chemical moiety called “polymerisation modulator”. The high molecular weight and the conformational flexibility around the centered modulator impart optimised flexibility and network structure to SDR® Bulk Fill Flowable Composite. The SDR® Bulk Fill Flowable Composite Technology can dissipate more energy during polymerisation, thereby inherently reducing the shrinkage stress. As a result, SDR® Bulk Fill Flowable Composite provides an approximately 20% reduction in volumetric shrinkage and almost an 80% reduction in polymerisation stress compared to conventional methacrylate resins.
Illustration of the SDR® Bulk Fill Flowable Composite monomer with a molecular weight of 849 g/mol compared to 513 g/mol for conventional Bis-GMA, and the modulator component. The high molecular weight and the conformational flexibility around the centered modulator impart optimised flexibility and network structure to SDR® Bulk Fill Flowable Composite.
Current SDR® Bulk Fill Flowable Composite Material characteristics
In comparison to the original chemistry, the resin matrix and filler paste have been modified in the currently available SDR® Bulk Fill Flowable Products (SDR® flow+ / SDR® Plus). The filler load has been increased by 2.5% to strengthen the material, improve its radiopacity and reduce its wear.
The previous glass filler has been partially replaced by an alternative filler which provides higher strength. The resin was also re-formulated to adjust to the overall consistency of the new filler loading and retain the flowability and self-leveling, key characteristics of SDR® Bulk Fill Flowable Composite. The patented and therefore unique characteristics of the first generation SDR® Bulk Fill Flowable Material were preserved while increasing the wear resistance to the level of standard flowable composites and the radiopacity by approximately 20% to 2.6mm Al.
Comparing SDR® Bulk Fill Flowable Composite:
In vitro Studies on Polymerisation Shrinkage and Marginal Adaptation
For in vitro studies, new technologies have been introduced to assess marginal adaptation of different types of composites in Class I and II posterior composite restorations. Microcomputed tomography (μ-CT) allows for non-destructive evaluation of the restorative interface in two and three dimensions and can measure volumetrically in microns the marginal integrity and internal adaptation of the restorative materials studied.8,19,27
A recent study28 evaluated three bulk-fill composite resins, including SDR® Bulk Fill Flowable, against a conventional composite resin in caries free and crack free human molars prepared with a MOD restoration. The teeth were thermocyled and cyclic loaded to mimic aging and stresses in the oral cavity during function. Micro-CT was performed on each sample to measure the interfacial gap at the restorative interface.
The results demonstrated that SDR® Bulk Fill Flowable had the smallest gap volume of all tested composite resins. An additional in vitro Micro-CT study19 on Class I restorations concluded SDR® Bulk Fill Flowable exhibited less volumetric polymerisation shrinkage compared with the other flowable groups.
Swept-Source Optical Coherence Tomography (SS-OCT) is another in vitro technology developed to visualise how composites behave while undergoing light polymerisation using real-time video display. Two studies29,30 concluded SDR® Bulk Fill Flowable Composite had a slower polymerisation rate and a delayed gel point of resin matrix increasing its flow capacity as demonstrated by a lower incidence of voids and better internal dentine adaptation at both 2mm and 4mm depths compared to a conventional flowable composite. Another SS-OCT study31 demonstrated that SDR® Bulk Fill Flowable Composite had a low shrinkage stress making it ideal as an intermediate dentine replacement layer for better internal adaptation compared to other bulk-fill composites.
A biocompatibility study32 found that only SDR® Bulk Fill Flowable and one other bulk fill composite demonstrated cell viability above 70% at a 4mm increment, whereas two standard composites, two bulk-fill pre-reacted glass ionomer composites and one other bulk-fill composite showed lower cell viability.
In studies assessing the degree of conversion and depth of cure when light curing bulk fill composites, SDR® Bulk Fill Flowable material showed significantly higher conversion degrees at the bottom and top surface than the other composites tested. Shorter curing times (10 seconds) significantly reduced the polymerisation of competitor materials. SDR® Bulk Fill Flowable demonstrated high polymerisation in 4mm thick bulks reaching the conversion degree of 2mm thick composite layers. SDR® Bulk Fill Flowable, in the manufacturer’s light-curing time, cured properly in 4mm. Higher radiant exposure of SDR® Bulk Fill Flowable had no adverse effect on its polymerisation shrinkage. Flowable bulk-fill composites like SDR® Bulk Fill Flowable performed better regarding polymerisation efficiency at 10 seconds compared to high viscosity bulk-fill composites that required 20 seconds.33,34,35,36
The Benefits of SDR® Bulk Fill Flowable Composite for Class II Restorations
At the onset of research on SDR® Bulk Fill Flowable Composite, several studies demonstrated its ability to bond well to the cavity floor in high C-factor restorations at 4mm increments.24,25,26 In the direct Class II posterior composite restoration, the goal for the clinician is to apply materials that reduce polymerisation shrinkage and shrinkage stress and work effectively on enamel, as well as in the proximal box of deep restorations where dentine and cementum become primary concerns for long-term success. Therefore, the type of composite resin used in the proximal box may play a critical role in the marginal adaptation of a Class II posterior composite restoration.
Using SDR® Bulk Fill Flowable Material in the open-sandwich technique for placement of a Class II posterior composite restoration allows a layer placed as dentine replacement extending from the gingival box floor up to 4mm. With the remaining top or enamel layer of at least 2mm, all proximal margins exposed to the oral cavity are sealed, which is of primary concern for long-term clinical success.
Clinical Trials and Results:
Retrospective and Randomised Controlled Studies
Clinical trials of Class II posterior composites published using SDR® Bulk Fill Flowable Material have been both retrospective and randomised controlled in methodology. A recent retrospective study37 of SDR® Bulk Fill Flowable Composite used in two increments as a 4mm dentine increment with a 2mm enamel layer of a traditional composite versus a traditional composite used in three 2mm increments resulted in the SDR® Bulk Fill Flowable group performing better over a 3-year period. The authors concluded the use of SDR® Bulk Fill Flowable Composite may provide a reduced procedure time for posterior composites over conventional composites and extended incremental techniques.
4-year randomised prospective split-mouth evaluation
A recent 4-year randomised prospective split-mouth evaluation of bulk fill flowable composites in Class II posterior composite restorations compared a conventional microhybrid composite resin against flowable bulk-fill and nanoparticulate composite resins, and flowable bulk-fill and microhybrid composite resins, (SDR® Bulk Fill Flowable + TPH®3 Composite, Dentsply Sirona). The results demonstrated that the SDR® Bulk Fill Flowable/ TPH®3 Composite group had better performance for wear and surface staining than the other groups.38
6-year randomised controlled study
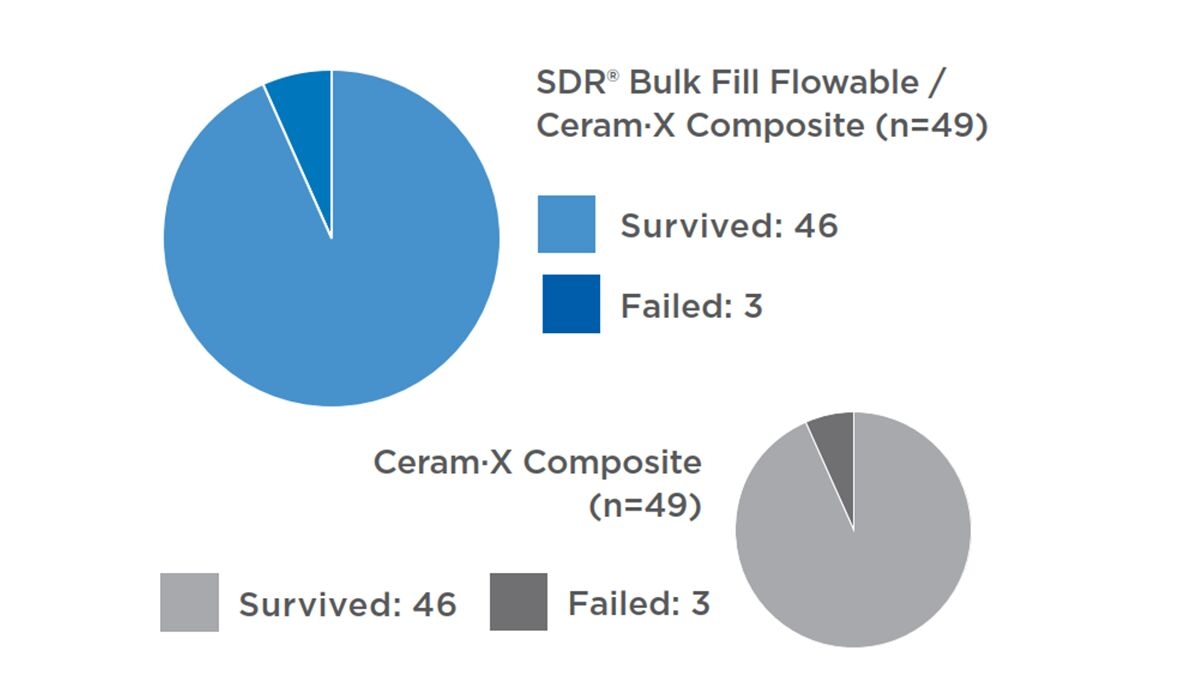
A 6-year randomised controlled study39 evaluated a flowable resin composite bulk-fill technique in posterior restorations and compared it with a conventional 2mm composite layering technique for Class I and II posterior composite restorations. Thirty-eight pairs of Class II restorations and 15 pairs of Class I restorations were placed in 38 adults. In the first cavity of each pair, the flowable resin composite (SDR® Bulk Fill Flowable) was placed, in bulk increments of up to 4mm. The occlusal aspect was finished with a layer of nanohybrid resin composite. In the second cavity of each pair, the hybrid resin composite was placed in 2mm increments. After 6 years, 72 Class II restorations and 26 Class I restorations could be evaluated. Six failed Class II molar restorations, three in each group, were observed, resulting in a success rate of 93.9% for all restorations and an annual failure rate (AFR) of 1.0% for both groups. The main reason for failure was resin composite fracture and not secondary caries.
6-year survival rates of Class I and II restorations filled with SDR® flow+ Bulk Fill Flowable and capped with a universal composite (Ceram•X® Nano Ceramic Restorative by Dentsply Sirona) in comparison to layered restorations in the same patients, using a universal composite (Ceram•X® Nano Ceramic Restorative by Dentsply Sirona).³⁹
The investigators were able to replicate those results in a 5-year randomised controlled study41 that followed a similar protocol with 38 pairs of Class I and 62 pairs of Class II restorations (first restoration with 4 mm SDR® Bulk Fill Flowable Composite + nano-hybrid resin, second restoration with nano-hybrid resin composite in 2mm increments) placed in 86 patients.
After 5 years, 68 Class I and 115 Class II restorations could be evaluated. Ten restorations failed with four in the SDR® Bulk Fill Flowable Composite and six in the control group due to tooth fracture and secondary caries, resulting in a success rate of 94.5% for all restorations and an annual failure rate (AFR) of 1.1% for the SDR® Bulk Fill Flowable group and 1.3% for the control group.
Conclusion:
SDR® Bulk Fill Flowable Composite as a Game-Changer in Dental Restorations
Developed in 2009, flowable bulk fill composites with SDR® Bulk Fill Flowable Composite technology became the first composite resin that allowed 4mm bulk placement in flowable nature. Now, over 13 years later, SDR® Bulk Fill Flowable Composite has established itself as the most important development in composite resin technology and biggest game changer for posterior composite restorations.
Improved Marginal Integrity, Reduced Shrinkage Stress, and Enhanced Longevity
The success of a Class II composite resin is dependent upon placing a material in the most constricted area of the restoration, the gingival box. Placement of SDR® Bulk Fill Flowable Composite not only seals that gingival margin better than conventional and other bulk fill composites but in combination with only 1-2 increments of the enamel top layer with a nano-hybrid composite can expedite the technique and oral environment sensitive procedure compared to traditional multiple small increment protocols.40
Many materials have tried to imitate the SDR® Bulk Fill Flowable Composite but no other dental material has been studied as extensively or ever duplicated the successful clinical results of over a hundred million restorations produced using SDR® Bulk Fill Flowable Composite technology. In vitro studies and clinical trials have clearly demonstrated that no other material available to dentists all over the world is better than SDR® Bulk Fill Flowable Composite as the true bulk fill dentine replacement material for every composite restoration.
SDR® flow+ White Paper
SDR® flow+ | White Paper Dr. Alan Atlas | EN | Europe
1. Bayne SC, Ferracane JL, Marshall GW, Marshall SJ, van Noort R. The Evolution of Dental Materials over the Past Century: Silver and Gold to Tooth Color and Beyond. J Dent Res. 2019 Mar;98(3):257-265
2. Worthington HV, Khangura S, Seal K, Mierzwinski-Urban M, Veitz-Keenan A, Sahrmann P, Schmidlin PR, Davis D, Iheozor-Ejiofor Z, Rasines Alcaraz MG. Direct composite resin fillings versus amalgam fillings for permanent posterior teeth. Cochrane Database Syst Rev. 2021 Aug 13;8(8):CD005620.
3. Bayne SC, Ferracane JL, Marshall GW, Marshall SJ, van Noort R. The Evolution of Dental Materials over the Past Century: Silver and Gold to Tooth Color and Beyond. J Dent Res. 2019 Mar;98(3):257-265.
4. Zorzin J, Maier E, Harre S, Fey T, Belli R, Lohbauer U, Petschelt A, Taschner M. Bulk-fill resin composites: polymerization properties and extended light curing. Dent Mater. 2015 Mar;31(3):293-301.
5. Ferracane JL, Hilton TJ. Polymerization stress--is it clinically meaningful? Dent Mater. 2016 Jan;32(1):1-10.
6. Demirel G, Baltacioglu IH, Kolsuz ME, Ocak M, Bilecenoglu B, Orhan K. Volumetric Cuspal Deflection of Premolars Restored With Different Paste-like Bulk-fill Resin Composites Evaluated by Microcomputed Tomography. Oper Dent. 2020 Mar/Apr;45(2):143-150. doi: 10.2341/19-019-L. Epub 2019 Jul 8. PMID: 31283421.
7. Versluis A, Tantbiroin D, Douglas WH. Do dental composites always shrink toward the light? J Dent Res 1998;77:1435-45
8. Van Ende A, Van de Casteele E, Depypere M, De Munck J, Li X, Maes F, Wevers M, Van Meerbeek B. 3D volumetric displacement and strain analysis of composite polymerization. Dent Mater. 2015 Apr;31(4):453-61
9. Rosatto CM, Bicalho AA, Veríssimo C, Bragança GF, Rodrigues MP, Tantbirojn D, Versluis A, Soares CJ. Mechanical properties, shrinkage stress, cuspal strain and fracture resistance of molars restored with bulk-fill composites and incremental filling technique. J Dent. 2015 Dec;43(12):1519-28
10. Bicalho AA, Valdívia AD, Barreto BC, Tantbirojn D, Versluis A, Soares CJ. Incremental filling technique and composite material--part II: shrinkage and shrinkage stresses. Oper Dent. 2014 Mar-Apr;39(2):E83-92.
11. Kim RJ, Kim YJ, Choi NS, Lee IB. Polymerization shrinkage, modulus, and shrinkage stress related to tooth-restoration interfacial debonding in bulk-fill composites. J Dent. 2015 Apr;43(4):430-9.
12. Kaisarly D, Langenegger R, Litzenburger F, Heck K, El Gezawi M, Rösch P, Kunzelmann KH. Effects of application method on shrinkage vectors and volumetric shrinkage of bulk-fill composites in class-II restorations. Dent Mater. 2022 Jan;38(1):79-93
13. Rizzante FAP, Mondelli RFL, Furuse AY, Borges AFS, Mendonça G, Ishikiriama SK. Shrinkage stress and elastic modulus assessment of bulk-fill composites. J Appl Oral Sci. 2019 Jan 7;27:e20180132.
14. Cerda-Rizo ER, de Paula Rodrigues M, Vilela A, Braga S, Oliveira L, Garcia-Silva TC, Soares CJ. Bonding Interaction and Shrinkage Stress of Low-viscosity Bulk Fill Resin Composites With High-viscosity Bulk Fill or Conventional Resin Composites. Oper Dent. 2019 Nov/Dec;44(6):625-636.
15. Ilie N, Hickel R. Investigations on a methacrylate-based flowable composite based on the SDR™ technology. Dent Mater. 2011 Apr;27(4):348-55.
16. Marovic D, Tauböck TT, Attin T, Panduric V, Tarle Z. Monomer conversion and shrinkage force kinetics of low-viscosity bulk-fill resin composites. Acta Odontol Scand. 2015 Aug;73(6):474-80.
17. Tauböck TT, Jäger F, Attin T. Polymerization shrinkage and shrinkage force kinetics of high- and low-viscosity dimethacrylate- and ormocer-based bulk-fill resin composites. Odontology. 2019 Jan;107(1):103-110.
18. Kim YJ, Kim R, Ferracane JL, Lee IB. Influence of the Compliance and Layering Method on the Wall Deflection of Simulated Cavities in Bulk-fill Composite Restoration. Oper Dent. 2016 Nov/Dec;41(6):e183-e194.
19. Sampaio CS, Chiu KJ, Farrokhmanesh E, Janal M, Puppin-Rontani RM, Giannini M, Bonfante EA, Coelho PG, Hirata R. Microcomputed Tomography Evaluation of Polymerization Shrinkage of Class I Flowable Resin Composite Restorations. Oper Dent. 2017 Jan/Feb;42(1):E16-E23.
20. Fronza BM, Rueggeberg FA, Braga RR, Mogilevych B, Soares LE, Martin AA, Ambrosano G, Giannini M. Monomer conversion, microhardness, internal marginal adaptation, and shrinkage stress of bulk-fill resin composites. Dent Mater. 2015 Dec;31(12):1542-51.
21. El-Damanhoury H, Platt J. Polymerization shrinkage stress kinetics and related properties of bulk-fill resin composites. Oper Dent. 2014 Jul-Aug;39(4):374-82. doi: 10.2341/13-017-L. Epub 2013 Jul 18. PMID: 23865582.
22. Han SH, Sadr A, Shimada Y, Tagami J, Park SH. Internal adaptation of composite restorations with or without an intermediate layer: Effect of polymerization shrinkage parameters of the layer material. J Dent. 2019 Jan;80:41-48.
23. Pereira R, Giorgi MCC, Lins RBE, Theobaldo JD, Lima DANL, Marchi GM, Aguiar FHB. Physical and photoelastic properties of bulk-fill and conventional composites. Clin Cosmet Investig Dent. 2018 Dec 12;10:287-296.
24. Van Ende A, De Munck J, Van Landuyt KL, Poitevin A, Peumans M, Van Meerbeek B. Bulk-filling of high C-factor posterior cavities: effect on adhesion to cavity-bottom dentin. Dent Mater. 2013 Mar;29(3):269-77.
25. Al-Harbi F, Kaisarly D, Michna A, ArRejaie A, Bader D, El Gezawi M. Cervical Interfacial Bonding Effectiveness of Class II Bulk Versus Incremental Fill Resin Composite Restorations. Oper Dent. 2015 Nov-Dec;40(6):622-35.
26. Shahidi C, Krejci I, Dietschi D. In Vitro Evaluation of Marginal Adaptation of Direct Class II Composite Restorations Made of Different “Low-Shrinkage” Systems. Oper Dent. 2017 May/Jun;42(3):273-283.
27. Rizzante FAP, Sedky RAF, Furuse AY, Teich S, Ishikiriama SK, Mendonça G. Validation of a method of quantifying 3D leakage in dental restorations. J Prosthet Dent. 2020 Jun;123(6):839-844.
28. Al Sheikh R. Marginal Adaptation of Different Bulk-fill Composites: A Microcomputed Tomography Evaluation. Oman Med J. 2022 Jan 31;37(1):e339.
29. Nazari A, Sadr A, Shimada Y, Tagami J, Sumi Y. 3D assessment of void and gap formation in flowable resin composites using optical coherence tomography. J Adhes Dent. 2013 Jun;15(3):237-43.
30. Nazari A, Sadr A, Saghiri MA, Campillo-Funollet M, Hamba H, Shimada Y, Tagami J, Sumi Y. Non-destructive characterization of voids in six flowable composites using swept-source optical coherence tomography. Dent Mater. 2013 Mar;29(3):278-86.
31. Han SH, Sadr A, Shimada Y, Tagami J, Park SH. Internal adaptation of composite restorations with or without an intermediate layer: Effect of polymerization shrinkage parameters of the layer material. J Dent. 2019 Jan; 80:41-48.
32. Toh WS, Yap AU, Lim SY. In Vitro Biocompatibility of Contemporary Bulk-fill Composites. Oper Dent. 2015 Nov-Dec;40(6):644-52.
33. Lempel E, Czibulya Z, Kovács B, Szalma J, Tóth Á, Kunsági-Máté S, Varga Z, Böddi K. Degree of Conversion and BisGMA, TEGDMA, UDMA Elution from Flowable Bulk Fill Composites. Int J Mol Sci. 2016 May 20;17(5):732.
34. Zorzin J, Maier E, Harre S, Fey T, Belli R, Lohbauer U, Petschelt A, Taschner M. Bulk-fill resin composites: polymerization properties and extended light curing. Dent Mater. 2015 Mar;31(3):293-301.
35. Miletic V, Pongprueksa P, De Munck J, Brooks NR, Van Meerbeek B. Curing characteristics of flowable and sculptable bulk-fill composites. Clin Oral Investig. 2017 May;21(4):1201-1212.
36. Pereira R, Giorgi MCC, Lins RBE, Theobaldo JD, Lima DANL, Marchi GM, Aguiar FHB. Physical and photoelastic properties of bulk-fill and conventional composites. Clin Cosmet Investig Dent. 2018 Dec 12;10:287-296.
37. Ugurlu M, Sari F. A 3-year retrospective study of clinical durability of bulk-filled resin composite restorations. Restor Dent Endod. 2021 Dec 30;47(1):e5.
38. Endo Hoshino IA, Fraga Briso AL, Bueno Esteves LM, Dos Santos PH, Meira Borghi Frascino S, Fagundes TC. Randomized prospective clinical trial of class II restorations using flowable bulk-fill resin composites: 4-year follow-up. Clin Oral Investig. 2022 May 13.
39. van Dijken JWV, Pallesen U. Bulk-filled posterior resin restorations based on stress-decreasing resin technology: a randomized, controlled 6-year evaluation. Eur J Oral Sci. 2017 Aug;125(4):303-309.
40. Sampaio CS, Garcés GA, Kolakarnprasert N, Atria PJ, Giannini M, Hirata R. External Marginal Gap Evaluation of Different Resin-filling Techniques for Class II Restorations-A Micro-CT and SEM Analysis. Oper Dent. 2020 Jul 1;45(4):E167-E175.
41. van Dijken JWV, Pallesen U. Posterior bulk-filled resin composite restorations: A 5-year randomized controlled clinical study. J Dent. 2016 Aug; 51:29-35.