Learn more about the Dentsply Sirona Windows 11 Security Package to continue ensuring security and compatibility of your Dentsply Sirona devices.
Class II Solution
Blog Post
Restorative
Regardless of the clinical situation, there is one thing that all endodontic treatments have in common: They need a high-quality coronal restoration to ensure long-term success and apical periodontal health. Ray and Trope1 found evidence on the strong link between marginal integrity of the coronal restoration and the absence of apical periodontitis back in 1995, which has been confirmed by several more recent studies2,3,4. When planning for an endodontic treatment, it therefore is paramount to also consider the appropriate type of coronal restoration, and the final choice for the case at hand might not always be the same.
This seems to go against the classic recommendation of always putting a crown on endodontically treated teeth but is actually in line with science. In their 2019 paper on evidence-based treatment planning for endodontically treated teeth5, Alan Atlas, Simone Grandini and Marco Martignoni conclude that “[…]with classic crowning, […] a significant amount of residual tooth structure is sacrificed in the preparation. Moreover, crowning often involves creating a subgingival perparation margin and therefore a significantly less hygienic margin region. For those reasons and in the light of recent research results, the almost habitual, reflex-like decision in favour of crowning single teeth regardless of the coronal cavity configuration must be considered questionable.”5
Among other options, a direct post-endodontic restoration might therefore be the treatment of choice to prevent unnecessary loss of tooth structure and complications during the restorative procedure. It also might cut the treatment cost for the patient by a significant amount, depending on local insurance- and health system. But are there viable options that ensure a long-term success of the endo treatment?
Scientific insights into direct post-endodontic restorations
Research indicates that the performance of direct post-endodontic treatments greatly depends on the amount and configuration of the remaining coronal tooth structure. A retrospective clinical investigation of 676 endodontically treated posterior teeth6 observed similar survival rates for crowns placed on a customised post and adhesive composite fillings in teeth with limited coronal damage. The authors concluded that “Cavities with up to three surfaces may well be successfully restored adhesively with composite filling material”6.
Figure 1: Clinical survival [years] of 676 endodontically treated posterior teeth and cavities with up to three surfaces
(three to four remaining walls) by Dammaschke T. aet al., 20136
![Figure 1 Clinical survival [years] of 676 endodontically treated posterior teeth and cavities with up to three surfaces (three to four remaining walls) by Dammaschke T. aet al., 2013 6](/en-gb/discover/discover-by-topic/by-category/restorative/direct-post-endo-restorations-with-tight-seal/_jcr_content/root/container/dentsplycontainer_114613258/image.coreimg.png/1739814550977/res-chart-sdr-dammaschke-2013-survival-rate-endo-class-i-and-ii.png)
This conclusion finds support in several other reviews and retrospective studies7,8, leading to the conclusion by Atlas aet al. that “[…] in ETT [endodontically treated teeth] with three or four coronal walls left, that is, at least one marginal ridge remaining, and no undermined cavity walls, direct adhesive restoration may be considered as an alternative to cuspal coverage.”5 Figure 2 provides a clinical example of both a Class I and II cavity in endodontically treated teeth, that are matching these criteria, allowing dental practitioners to place a less invasive and more cost effective direct restoration.
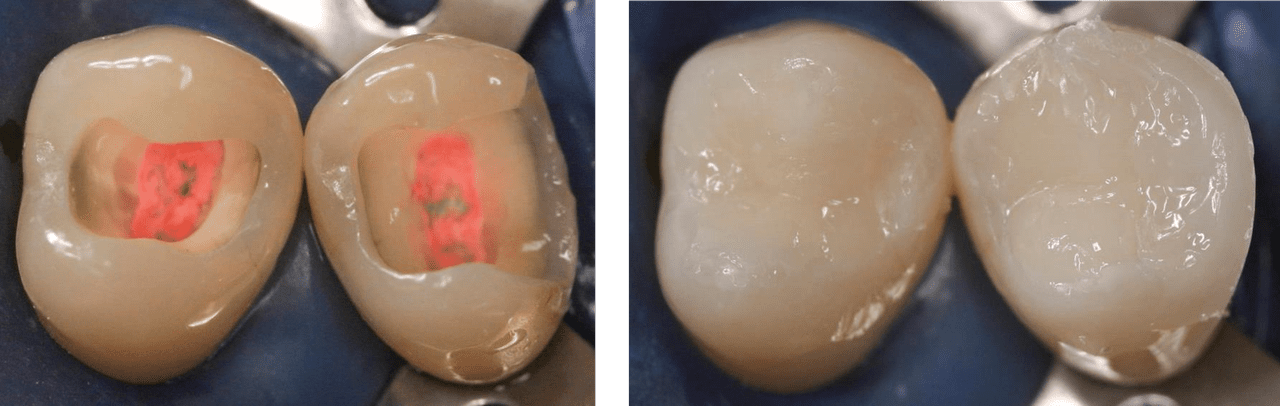
Figure 2: Endodontically treated posterior teeth with four and three coronal walls, and barely undermined residual tooth structure before and after direct restoration
(Courtesy of Dr. Marcus Holzmeier, Germany)
The real deal is a proper seal
Ray and Trope1 already highlighted the importance of maintaining marginal integrity of the coronal restoration for the long-term success of an endo and the prevention of apical periodontitis. Regarding direct post-endodontic restorations on posterior teeth, this means that dental practitioners are facing the same challenge as in Class I and II restorations on vital teeth: Preventing microleakage by achieving a proper seal and creating a gap-free restoration.
But because of their depth and shape, endodontic Class I and II cavities are even more challenging than regular posterior cavities. They require placement of more filling material than usual, and not only do so gap-free but also at the right layer thickness to ensure a proper management of shrinkage stress and maintain a seamless adaptation to the cavity walls during curing.
The importance of managing shrinkage stress through proper placement in post-endodontic restorations cannot be overstated, as most surfaces of a post-endodontic restoration are bonded to cavity walls. At the same time, the root canal orifices can make it difficult to determine the actual depth of the cavity and the layer thickness of already placed composite.
Figure 3: Large quantities of filling material need to be placed in posterior post-endodontic cavities
This can create significant shrinkage stress through the amount of bonded surfaces. In addition, it is hard to visually determine the depth of the cavity including root canal orifices, and place Universal Composites and Flowables in the right layer thickness (clinical picture by Paqué F., 2014).

SDR® flow+ Bulk Fill Flowable from Dentsply Sirona is an excellent choice to deal with the challenge of achieving a proper seal in post-endodontic restorations, as it provides an extremely low polymerisation stress as well as excellent flowability and self-levelling without manipulation. This not only mitigates the risk of creating too much shrinkage stress, but also makes material placement easier and can even save time during treatment. As shown in the clinical case below, placing two layers of SDR® flow+ composite can be enough to fill the bulk of the post-endodontic cavity.
Video provided by Dr. Peet van der Vyver, Johannesburg (South Africa), studio4endo.com.
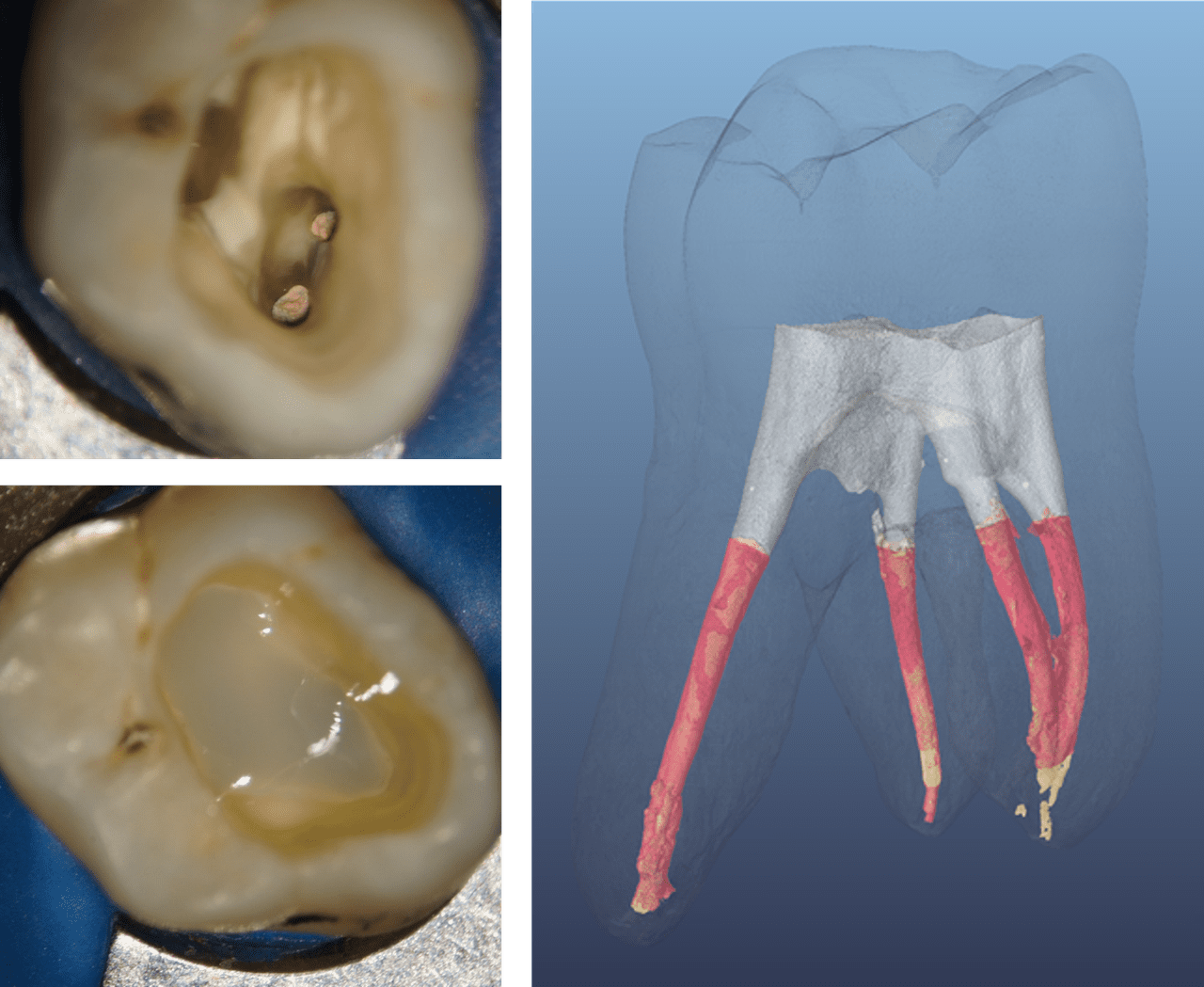
The result is a tightly sealed coronal restoration, as shown in the micro-CT image of Figure 4, which shows the adaptation of the initial SDR® flow+ composite layer in a post-endodontic Class I cavity. SDR® flow+ Bulk Fill Flowable has adapted itself seamlessly to both the cavity walls and the root canal obturation material, creating the ideal conditions to achieve a proper coronal seal.
Figure 4: Analysis of the initial SDR® flow+ composite layer in a post-endodontic Class I cavity, using a micro-CT.
The SDR® flow+ composite layer (grey) shows a tight seal to the cavity walls as well as an excellent adaptation to the obturation material (red). (Image source: Paqué F., 2014 (ref. 14.1483))
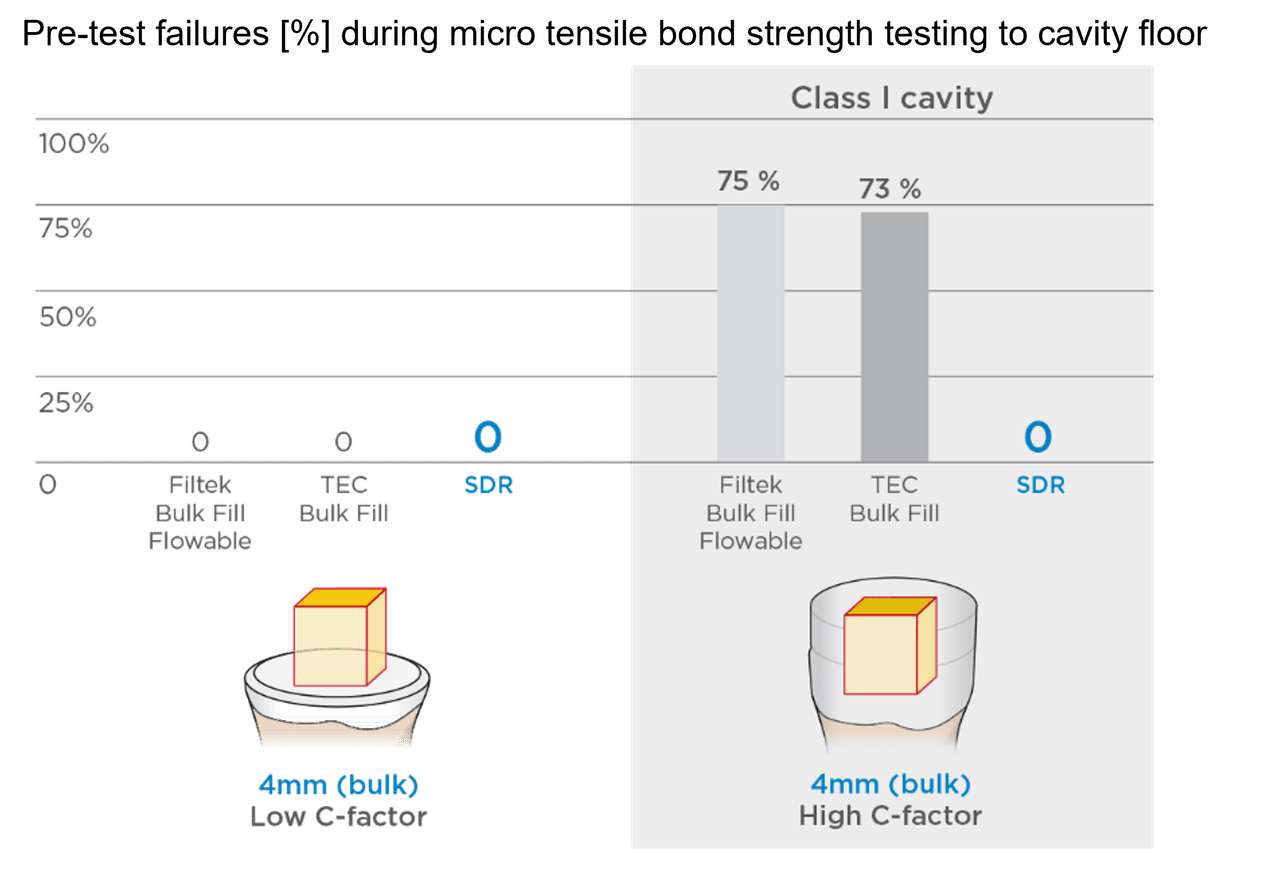
Dealing with shrinkage stress works equally well, when using SDR® flow+ Bulk Fill Flowable, as the SDR® bulk fill technology enables the formation of a more relaxed network, minimising the build-up of stress. This low-stress chemistry is able to deal even with the large amount of bonded surfaces in a post-endodontic cavity, as Van Ende9 has shown in 2016, proving that SDR® bulk fill flowable technology can deal with high C-factors, leading to a tight coronal seal even for post-endodontic cavities.
Figure 5: Shrinkage stress: Shown as a ratio of SDR® flow+ Bulk Fill Flowable in comparisson with other Direct Restoratives10

Tetric EvoFlow, x-tra Base, Filtek Bulk Fill Posterior, Filtek Supreme XT, SonicFill, Tetric EvoFlow Bulk Fill, Venus Bulk Fill and Filtek Bulk Fill Flowable are not registered trademarks of Dentsply Sirona.
Figure 6: Micro tensile bond strength testing on a flat surface v.s. a cavity with high C-factor similar to a post-endodontic Class I. While the other bulk fill materials in this in-vitro study showed high pre-test failure rates, the SDR® technology succeeded in dealing with the high shrinkage stress of the cavity with high C-factor.9
Create direct post-endodontic restorations with a tight seal
There are many reasons that can make direct coronal restorations the go-to option in an endodontic treatment – from the desire to preserve as much of the natural tooth as possible to financial considerations by the patient. And given the right clinical situation of a posterior Class I or II with three or more cavity walls remaining, scientific data indicates that this treatment option can lead to high quality outcomes with long-term success.

SDR® flow+
Create direct post-endodontic restorations with a tight seal
Achieving a proper coronal seal by creating gap-free adaptation and managing shrinkage stress however is paramount to reach that goal, and what would be a better material to get there than one that also makes placement faster and easier: SDR® flow+ Bulk Fill Flowable from Dentsply Sirona.
Please contact a Dentsply Sirona representative to find out more about SDR® flow+ Bulk Fill Flowable.
Explore Related Products






- Ray HA, Trope M. Periapical status of endodontically treated teeth in relation to the technical quality of the root filling and the coronal restoration. Int Endod J. 1995 Jan;28(1):12-8. doi: 10.1111/j.1365-2591.1995.tb00150.x. PMID: 7642323.
- Salehrabi R, Rotstein I. Endodontic treatment outcomes in a large patient population in the USA: an epidemiological study. J Endod. 2004 Dec;30(12):846-50. doi: 10.1097/01.don.0000145031.04236.ca. PMID: 15564861.
- Lynch CD, Burke FM, Ní Ríordáin R, Hannigan A. The influence of coronal restoration type on the survival of endodontically treated teeth. Eur J Prosthodont Restor Dent. 2004 Dec;12(4):171-6. PMID: 15691191.
- Gillen BM, Looney SW, Gu LS, Loushine BA, Weller RN, Loushine RJ, Pashley DH, Tay FR. Impact of the quality of coronal restoration versus the quality of root canal fillings on success of root canal treatment: a systematic review and meta-analysis. J Endod. 2011 Jul;37(7):895-902. doi: 10.1016/j.joen.2011.04.002. Epub 2011 May 24. PMID: 21689541; PMCID: PMC3815527.
- Atlas A., Grandini S., Martignoni M., 2019: Evidence-based treatment planning for the restoration of endodontically treated single teeth: importance of coronal seal, post vs no post, and indirect vs direct restorations, Quintessence Int 2019;50:772-781; 10.3290/j.qi.a43235
- Dammaschke T, Nykiel K, Sagheri D, Schäfer E. Influence of coronal restorations on the fracture resistance of root canal-treated premolar and molar teeth: a retrospective study. Aust Endod J. 2013 Aug;39(2):48-56. doi: 10.1111/aej.12002. Epub 2012 Dec 12. PMID: 23890259.
- Suksaphar W, Banomyong D, Jirathanyanatt T, Ngoenwiwatkul Y. Survival rates against fracture of endodontically treated posterior teeth restored with full-coverage crowns or resin composite restorations: a systematic review. Restor Dent Endod. 2017 Aug;42(3):157-167. doi: 10.5395/rde.2017.42.3.157. Epub 2017 Jul 31. PMID: 28808632; PMCID: PMC5553015.
- Lempel E, Lovász BV, Bihari E, Krajczár K, Jeges S, Tóth Á, Szalma J. Long-term clinical evaluation of direct resin composite restorations in vital vs. endodontically treated posterior teeth - Retrospective study up to 13 years. Dent Mater. 2019 Sep;35(9):1308-1318. doi: 10.1016/j.dental.2019.06.002. Epub 2019 Jul 2. PMID: 31278018.
- Van Ende A, De Munck J, Van Landuyt K, Van Meerbeek B. Effect of Bulk-filling on the Bonding Efficacy in Occlusal Class I Cavities. J Adhes Dent. 2016;18(2):119-24. doi: 10.3290/j.jad.a35905. PMID: 27042703.
- Internal data on file. For more information, contact Consumables-Data-Requests@dentsplysirona.com
