
Learn more about the Dentsply Sirona Windows 11 Security Package to continue ensuring security and compatibility of your Dentsply Sirona devices.


Infection prevention protocols in the operatory
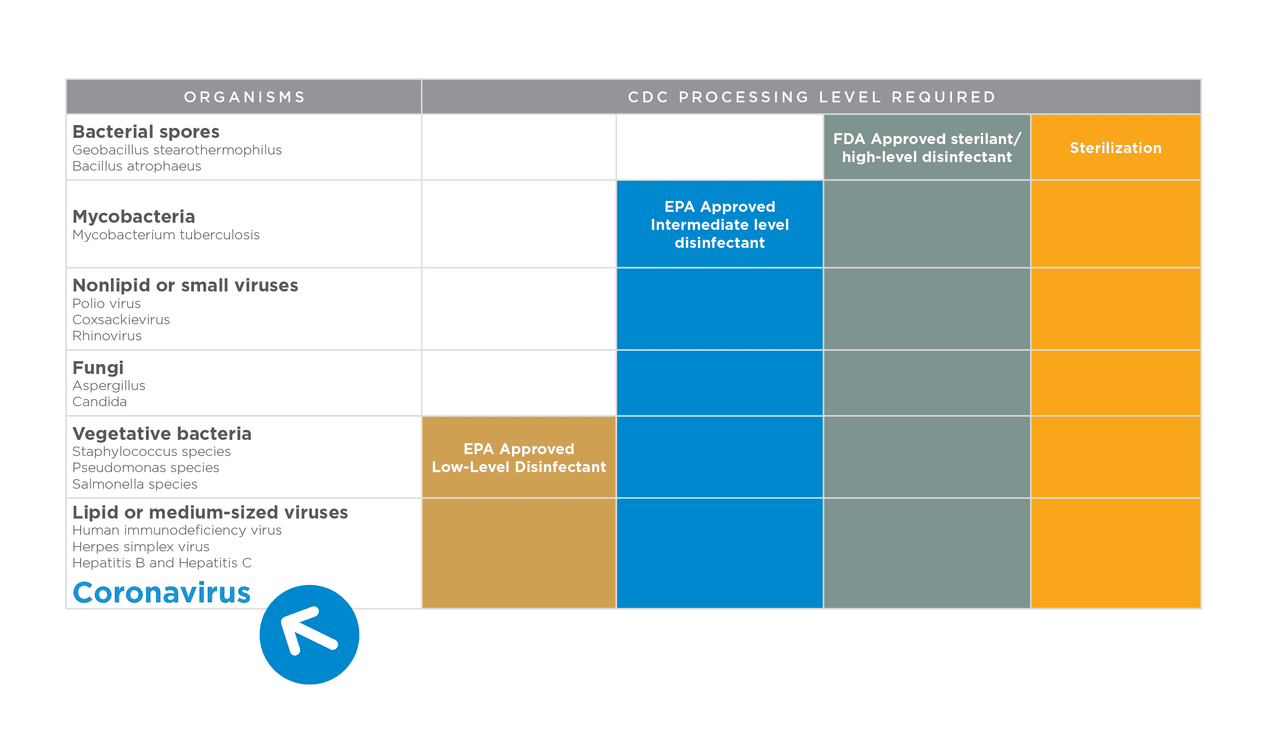
The Centers for Disease Control and Prevention (CDC) recommends dental offices follow an infection prevention protocol. This includes a focus around the safety of both patients and clinicians; the dental operatory is at the center of this focus.
Some important sterilization elements to consider in high-level prevention protocols are:
- Hand Hygiene
- Surface Disinfection
- Equipment Preparation
- Single-Use Disposables
- Aerosol Management
- Evacuation Systems
The recommendations below regarding these elements are summarized from CDC official guidelines.
Hand hygiene is the single most important measure to prevent the spread of infections among patients and clinicians.
Best practices for effective hand hygiene and reducing the risk of transmission
- No rings, watches, or jewelry
- Fingernails should be short with smooth, filed edges
- No artificial or painted fingernails
Recommended equipment for effective hand hygiene
- Automatic touch-free faucets
- Disposable towels
- Touch-free dispensers
- Plain soap
- Antimicrobal soap
- Alcohol-based hand rub
- Hand care products - lotions
When to perform hand hygiene
- When hands are visibly soiled
- After barehanded touching of contaminated instruments or surfaces
- Before or after treating each patient
- Before putting on gloves and again immediately after removing gloves
Dental units and equipment are complex systems. Key maintenance may be overlooked when performance is adequate. Maintenance will not only keep equipment at its peak but also protect you and your patients.
After a period of non-use or storage, dental equipment may require maintenance and/or repair. It is important to review the specific manufacturer's instructions for use (IFU) for all equipment and devices. Some considerations for equipment maintenance may include testing, shocking and/or treatment of dental unit waterlines.
Dental Unit Waterlines
"Dental unit waterlines (ie, plastic tubing that carries water to the high-speed handpiece, air/water syringe and ultrasonic scaler) promote bacterial growth and development of biofilm due to the presence of long narrow-bore tubing, inconsistent flow rates and the potential for retraction of oral fluids. Dental healthcare personnel and patients could be placed at risk of adverse health effects if water is not appropriately treated." 2
Dental Unit Waterline Considerations
- Follow the facility's dental unit waterline maintenance protocol
- Policies and protocols have not been established, create program and train all staff
"All dental units should use systems that treat water to meet drinking water standards (ie, ≤ 500 CFU/mL of heterotrophic water bacteria). Independent reservoirs—or water-bottle systems—alone are not sufficient." 3
- Consult with the dental unit and/or waterline treatment product manufacturer for appropriate methods and equipment to monitor and maintain the quality of dental water.
Other Recommendations
Replace/change water filters on devices containing removable filters on devices containing removable filters such as those found on ultrasonic scaling units
"CDC recommends that all dental instruments that use water should be run to discharge water for 20-30 seconds after each patient and for several minutes before the start of each clinic day." 4
Additional Maintenance Suggestions
Single-use disposables, also called single-use devices, are designed for use on one patient and then must be discarded. Examples of single-use devices include saliva ejectors, masks, prophylaxis angles, disposable barriers and air/water syringe tips.
According to the Food and Drug Administration a single-use device, also referred to as a disposable device, is intended for use on one patient during a single procedure. It is not intended to be reprocessed (i.e., cleaned and disinfected or sterilized) and used on another patient. The labeling may not identify the device as single-use or disposable. If a device does not have reprocessing instructions, regardless of labeling, it should be considered single-use and disposed of appropriately (i.e., according to federal, state, and local regulations) after one use.5 Using disposable items improves patient safety by eliminating the risk of patient-to-patient contamination.5
Considerations for surface barriers:
- Utilize disposable barriers to protect clinical contact surfaces that are difficult to clean (eg, switches on dental chairs, computer equipment) Change surface barriers between patients and then clean and disinfect surfaces.5,6
Considerations for air/water syringe tips:
- Narrow internal lumens of metal air/water syringe tips may be difficult to clean and sterilize effectively.
- Utilizing disposable air/water syringe tips reduce the risk of potential contamination.
Dental studies show:
"During dental treatments bacterial aerosols increase 5x7 and aerosols can spread up to eight feet.” 8
High-speed handpieces, ultrasonic scalers, air polishers and air/water syringes produce potentially infectious droplets, splatter and aerosols. DHCP should utilize a multi-layered approach in order to minimize the risk of cross-contamination in a dental setting.
1. Personal Protective Equipment (PPE)
- DHCP should don appropriate PPE as recommended in current guidelines and/or state regulations.
- Taking precautions to isolate the oral cavity with the placement of a rubber dam during restorative procedures may also reduce the aerosol production.
2. Pre-procedural mouth rinse
- Despite the lack of scientific evidence per CDC Guidelines, clinicians may use their professional judgment to use a pre-procedural virucidal mouth-rinse in order to sanitize the aerosol.
3. High-volume evacuation
- Using HVE instead of standard saliva ejectors is an important component to reduce the amount of aerosol.
- Several studies published show that utilizing HVE can reduce the amount of aerosol by 90%-98%.9
————————————————————————————————————————————————————
"The ADA recommends that all blood-contaminated aerosols and splatter should be minimized" 10
OSHA standards state that, "all procedures involving blood or other potentially infectious materials shall be performed in such a manner as to minimize splashing, spraying, splattering, and generation of droplets of these substances." 11
In the CDC guidelines for infection control in dental settings, the use of HVEs are considered to be 'appropriate work practices' - precautions that always should be followed during dental procedures.12

Purevac High Volume Evacuation System
In the dental setting, an evacuation system is an essential component for many dental procedures and maintaining the flow in a dental practice.

Explore more infection control & prevention topics
1. https://www.cdc.gov/infection-control/hcp/environmental-control/environmental-services.html
2. https://www.cdc.gov/dental-infection-control/hcp/summary/dental-unit-water-quality.html
3. CDC Recommendations for Dental Water Quality: The Centers for Disease Control and Prevention (CDC) Guidelines for Infection Control in Dental Settings 2003, which is derived from the U.S. EPA's Surface Water Treatment Rule.
4. https://www.cdc.gov/agricultural-water/about/index.html
5. https://www.cdc.gov/oralhealth/infectioncontrol
6. https://www.cdc.gov/dental-infection-control/hcp/dental-ipc-faqs/single-use-devices.html
7. Al Maghlouth A, Al Yousef Y, Al Bagieh N. Qualitative and Quantitative Analytics of Bacterial Aerosols. J Contemp Dent Pract 2004 November; (5)4:091-100.
8. Milejczak CB. Optimum Travel Distance of Dental Aerosols in the Dental Practice. J Dent Hyg. 2005 October;81(4):20-21
9. Jacks MJ: A laboratory comparison of evacuation devices on aerosol reduction. J Dent Hyg. 2002, 76, 202. Harrel SK, Barnes JB, Rivera-Hidalgo F. Reduction of aerosols produced by ultrasonic scalers. J Periodontal. 1996;67:28-32. Kyln SL, Cummings DE, Richardson BW, Davis RD. Reduction of bacteria-containing spray produced during ultrasonic scaling. Gen Dent. 2001;49(6):648-652
10. INFECTION CONTROL RECOMMENDATIONS FOR THE DENTAL OFFICE AND THE DENTAL LABRATORY The Journal of the American Dental Association, Volume 127, Issue 5, 672-680
11. https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.1030
12. The Centers for Disease Control and Prevention (CDC) Guidelines for Infection Control in Dental Settings 2003
13. Centers for Disease Control and Prevention. Summary of Infection Prevention Practices in Dental Settings: Basic Expectations for Safe Care. Atlanta, GA: Centers for Disease Control and Prevention, US Dept of Health and Human Services: October 2016
The infection control and prevention recommendations presented in this document are in alignment with the Centers for Disease Control and Prevention (CDC), and the Occupational Safety and Health Administration (osha).
The Organization for Safety Asepsis and Prevention (OSAP), provides many resources for DHCP which may be found on their website at OSAP.org.
The information provided does not, and is not intended to, constitute legal advice; instead, all information, content, and materials cited in this paper are for general informational purposes only. Information in this paper may not constitute the most up-to-date advisory, legal or other information. This paper contains citations to third-party publications and websites. Such references are only for the convenience of the reader. Readers should consult their own legal and other advisors for specific information impacting their practices.
